Muscle Pain Misdiagnosed as Tooth Pain — Root Canal Avoided

Patient Profile
South Bay patient presenting with ear ache and gum irritation from two weeks prior, referred for root canal evaluation
Clinical Challenge
Differentiating between true dental pathology and referred pain from muscle tightness in the masseter area
Approach
Thorough clinical examination, CBCT-guided assessment, and muscle massage recommendations
Outcome
Symptoms resolved with non-invasive muscle exercises, avoiding unnecessary root canal treatment
Treatment Details
The patient presented with a history of ear ache and gum irritation from approximately two weeks prior. They had been referred by their general dentist for root canal evaluation after reporting discomfort in the lower right quadrant. By the time of the specialist consultation, the acute symptoms had largely resolved—an important diagnostic clue.
Clinical Examination Findings
A systematic clinical examination revealed:
- No pain on palpation of any teeth in the affected quadrant
- No tooth mobility—all teeth tested within normal limits
- No signs of swelling or intraoral soft tissue abnormality
- Normal pulp vitality testing—all teeth responded normally to cold and electric pulp testing
- Slight tenderness on palpation of the masseter muscle—reproducible discomfort when pressure was applied to the muscle body
CBCT Assessment
A CBCT scan was obtained to definitively rule out dental pathology. The three-dimensional imaging confirmed:
- No periapical radiolucencies on any teeth in the region
- No evidence of fractures, cracks, or resorptive lesions
- Intact lamina dura and normal periodontal ligament space
- No pathology that would warrant endodontic intervention
Diagnosis: Myofascial Referred Pain
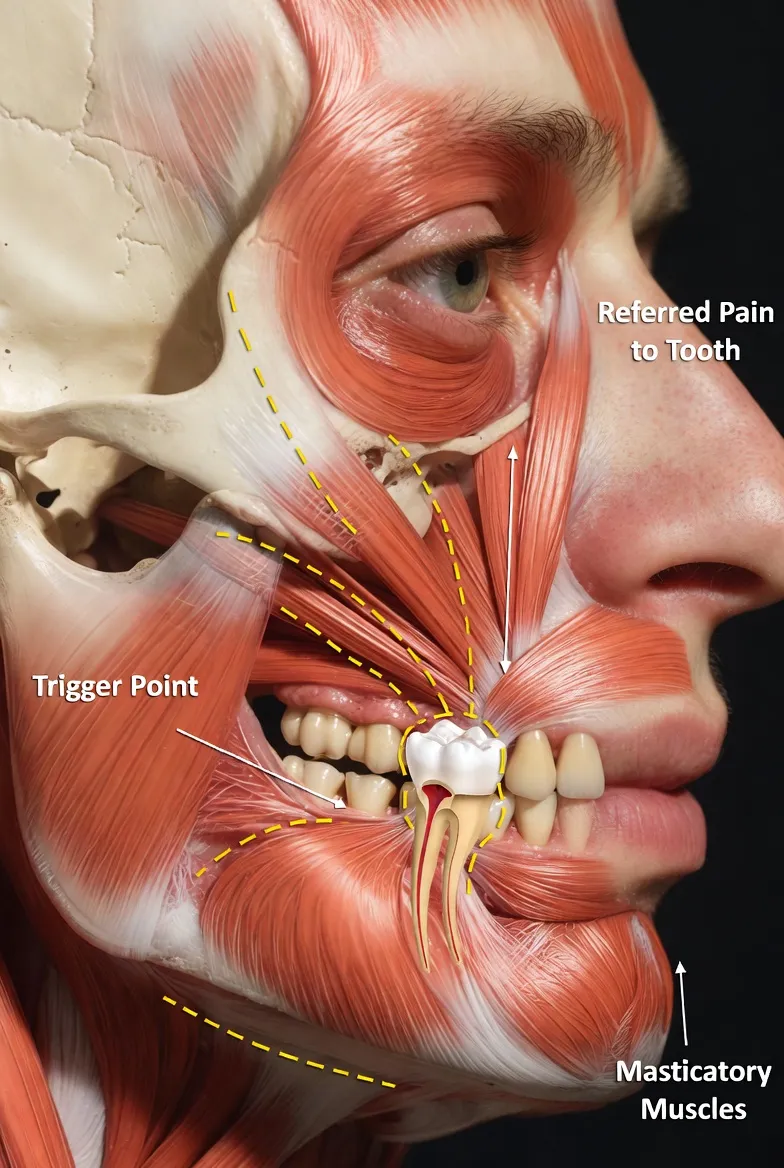
With dental pathology confidently ruled out, the diagnosis pointed to myofascial pain originating from the masseter muscle. The masseter—the primary muscle of mastication—can refer pain to the teeth, ear, and temporomandibular joint when it develops trigger points or chronic tightness from clenching or bruxism.
The patient was guided on targeted massage techniques for the masseter muscles and advised on stress reduction strategies. At 3-month follow-up, all symptoms had completely resolved without any dental treatment.
Clinical Assessment
This case illustrates one of the most important roles of specialist consultation: knowing when NOT to treat. The patient was on a pathway toward an invasive, irreversible procedure on a healthy tooth. A 30-minute specialist examination changed that outcome entirely.
Why Misdiagnosis Happens
Referred pain from the muscles of mastication is a well-documented phenomenon that mimics dental pathology:
- Masseter trigger points can refer pain to the lower molars, premolars, and even the ear—exactly where this patient reported symptoms
- Temporal muscle tightness can mimic pain in the upper teeth
- Symptoms can be intermittent, making them appear consistent with pulpitis (which also fluctuates)
- Radiographic ambiguity—2D radiographs sometimes show shadows that are misinterpreted as pathology
The Diagnostic Approach That Made the Difference
Several specific steps prevented an unnecessary root canal:
- Comprehensive vitality testing: All teeth responded normally—a healthy pulp does not need treatment
- CBCT imaging: Three-dimensional views eliminated the ambiguity inherent in 2D radiographs
- Extraoral muscle palpation: Reproducing the patient's symptoms by pressing on the masseter confirmed the myofascial origin
- Clinical correlation: The fact that symptoms had already begun resolving before any dental treatment was a strong indicator against irreversible pulpitis
The Cost of Getting It Wrong
Had a root canal been performed on the suspected tooth:
- The patient would have undergone an unnecessary invasive procedure on a healthy tooth
- The original symptoms would have persisted (since the source was muscular, not dental)
- The patient may have been subjected to additional procedures—possibly extraction—when the "root canal failed"
- Healthy tooth structure would have been permanently compromised
Key Takeaways
Clinical Insights
- Not all tooth pain comes from teeth: Myofascial pain, referred pain from the TMJ, sinusitis, and even neuralgia can all mimic dental pathology. A thorough differential diagnosis is essential before committing to irreversible treatment.
- Vitality testing is non-negotiable: A tooth that responds normally to cold testing has a living, healthy pulp. Root canal treatment on a vital tooth without clear pathology is unnecessary and harmful.
- CBCT resolves ambiguity: When 2D radiographs are inconclusive, three-dimensional imaging provides definitive answers. The cost of a CBCT scan is trivial compared to the cost of treating the wrong tooth.
- Resolving symptoms are a diagnostic clue: Irreversible pulpitis does not spontaneously improve. If a patient's pain is decreasing without treatment, consider non-dental etiologies.
- Specialist consultations save teeth: The value of a specialist isn't just in treating complex cases—it's also in recognizing when treatment isn't needed.
When to Suspect Myofascial Pain Over Dental Pathology
- Pain is diffuse rather than localized to a specific tooth
- Symptoms fluctuate with stress, clenching, or jaw activity
- All vitality tests are normal
- Radiographs show no convincing pathology
- Pain can be reproduced by pressing on the muscles of mastication
- Patient reports associated symptoms: ear ache, headache, jaw stiffness
Bottom Line: The best endodontic treatment is sometimes no treatment at all. A comprehensive specialist examination can save patients from unnecessary procedures, preserve healthy tooth structure, and resolve symptoms through conservative management.
Clinical Disclaimer: These cases are presented for educational purposes and published with appropriate patient consent. Patient identifying information has been removed in compliance with HIPAA regulations. Individual results may vary. All radiographic images and case descriptions represent actual patient treatment outcomes.
Procedures We Use for These Cases
The expertise demonstrated in these cases comes from mastering advanced endodontic procedures
Related Articles
Learn more about these treatments from Dr. Phan
 Cracked Teeth
Cracked Teeth Cracked Tooth: Crown, Root Canal, or Extraction? How We Decide
Not all cracked teeth need the same treatment. Dr. Jason Phan explains the 5 types of cracks, which ones can be saved, and how a microscope and CBCT determine the right treatment.
 Surgery & Retreatment
Surgery & Retreatment Failed Root Canal: Should You Try Retreatment or Get an Implant?
Your root canal didn't work — now what? Dr. Jason Phan compares retreatment vs. extraction and implant: success rates, costs, timelines, and how to decide which is right for your tooth.
Root Canal Root Canal vs. Implant: Which Is the Better Investment for Your Tooth?
Choosing between saving your tooth with a root canal or extracting and replacing it with an implant? Dr. Jason Phan compares cost, success rates, timelines, and long-term outcomes.
 Root Canal
Root Canal Persistent Pain After Root Canal: Causes, Evidence, and When Retreatment Is Needed
A detailed clinical guide to understanding why pain persists after root canal treatment. Dr. Jason Phan covers odontogenic and nonodontogenic causes, diagnostic approaches, and evidence from current research.
 Consultation
Consultation What Happens During an Endodontic Consultation
Nervous about seeing an endodontist? Dr. Jason Phan walks you through exactly what happens during a consultation at our Torrance office — from the exam to the treatment plan.
 Pain Diagnosis
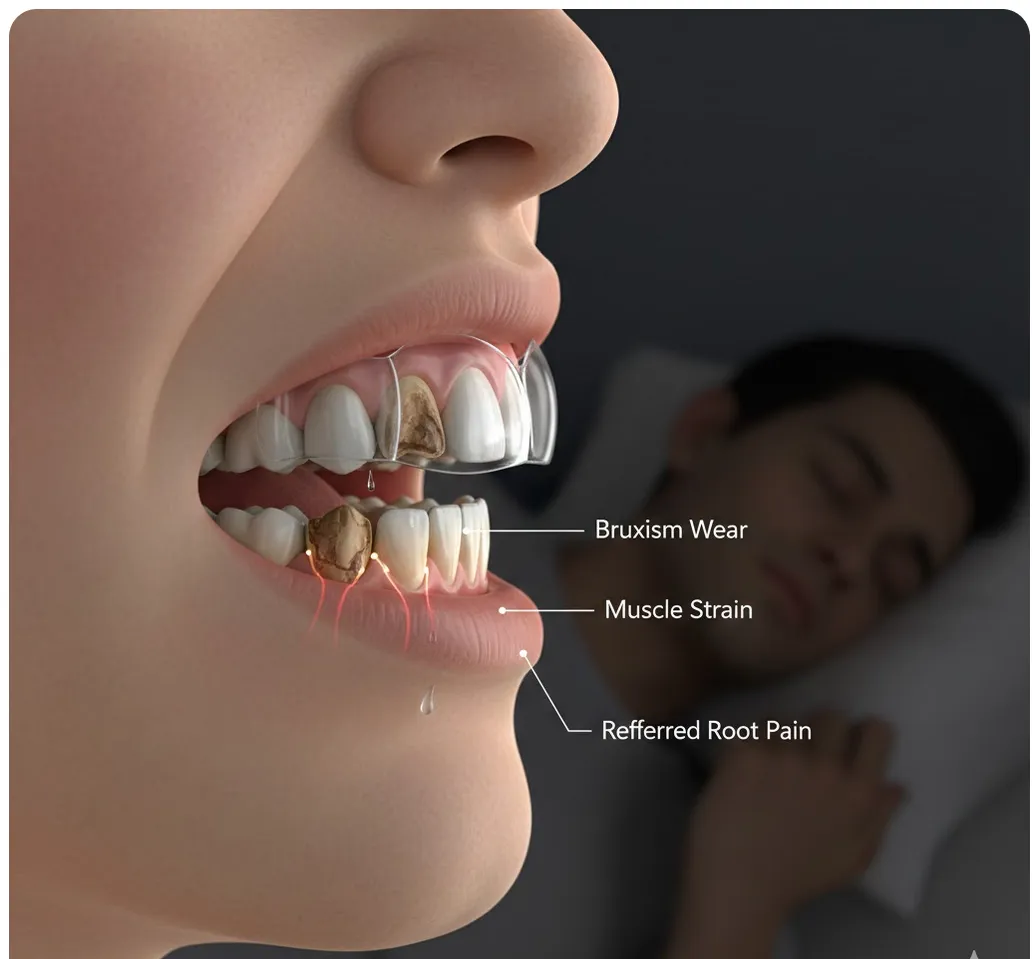
Pain Diagnosis Bruxism Pain Mimicking Root Canal Pain: When Grinding Feels Like a Toothache
Teeth grinding and clenching can cause tooth pain that mimics root canal symptoms. Dr. Jason Phan explains how a CBCT consultation in Torrance prevents unnecessary treatment.
 Pain Diagnosis
Pain Diagnosis Myofascial Pain Mimicking Root Canal Pain: When Jaw Muscles Cause Toothaches
Jaw muscle trigger points can refer pain to teeth, mimicking a root canal problem. Dr. Jason Phan explains how a detailed CBCT consultation in Torrance prevents misdiagnosis.
 Pain Diagnosis
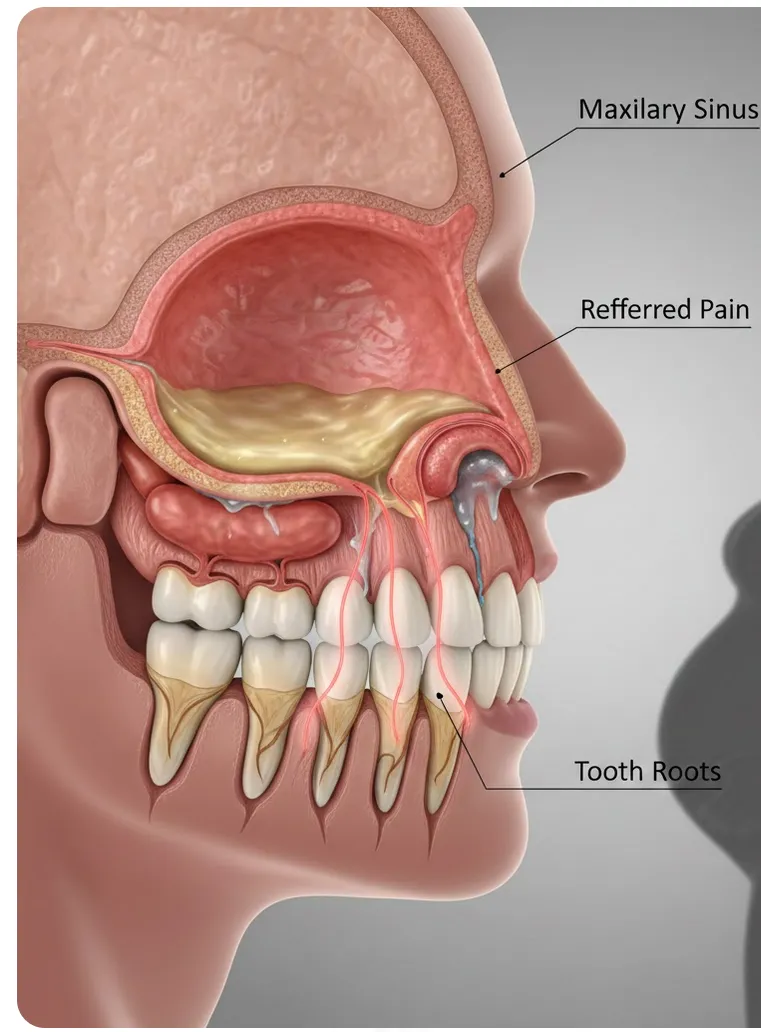
Pain Diagnosis Sinus Pain Mimicking Root Canal Pain: How to Tell the Difference
Maxillary sinusitis can cause tooth pain that feels like a root canal is needed. Dr. Jason Phan explains how CBCT imaging and thorough evaluation in Torrance prevent misdiagnosis.
 Pain Diagnosis
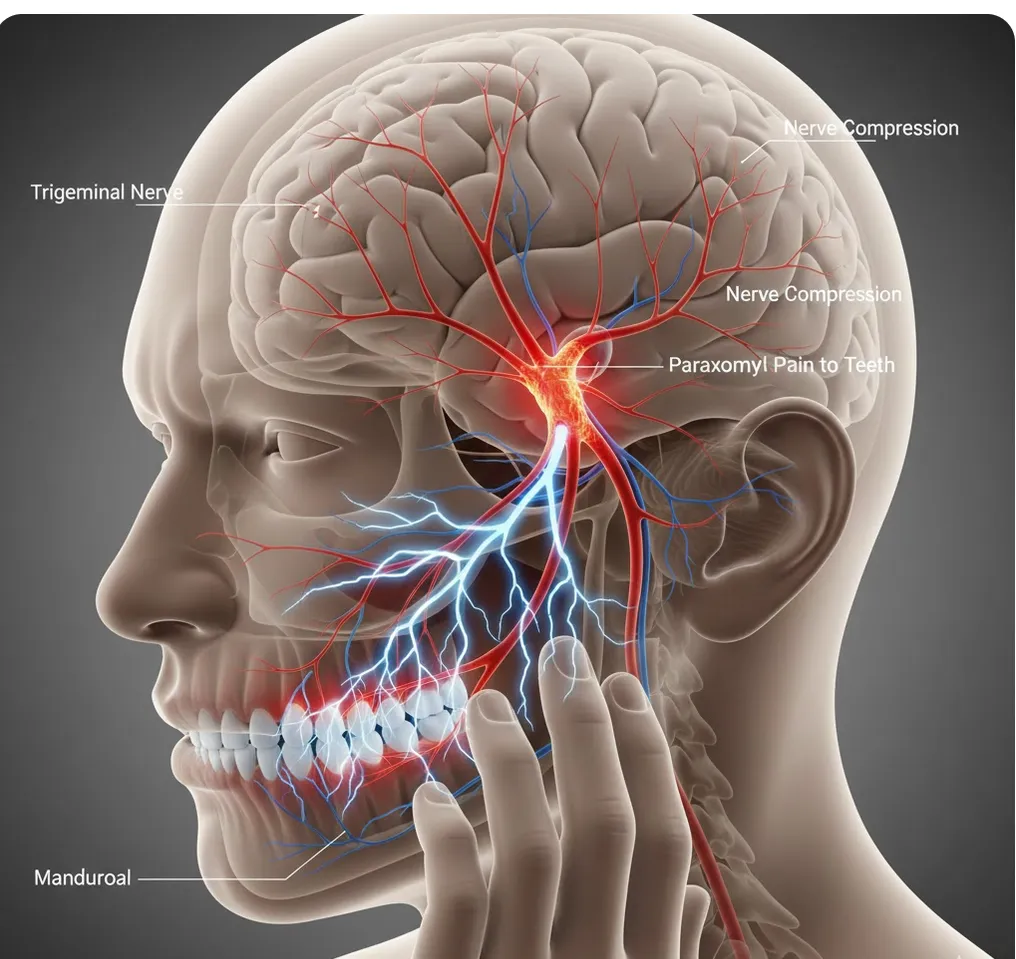
Pain Diagnosis Trigeminal Neuralgia & Other Nerve Conditions Mimicking Root Canal Pain
Trigeminal neuralgia causes intense facial pain often misdiagnosed as tooth problems. Dr. Jason Phan explains how CBCT consultation in Torrance prevents unnecessary root canals.
 Root Canal
Root Canal Endodontist vs. Dentist for Root Canal: 95% vs. 85% Success Rate
Endodontists have a 95–97% root canal success rate vs. 85–90% for general dentists. See the full comparison of training, equipment, cost, and when the specialist difference matters most.
 Pain Diagnosis
Pain Diagnosis Shingles Presenting as Tooth Pain: What You Need to Know
Shingles can mimic tooth pain, leading to unnecessary dental procedures. Dr. Jason Phan explains how herpes zoster affects the trigeminal nerve, the signs to watch for, and when to seek treatment.
Experience Matters in Complex Endodontics
When you refer patients to us, they benefit from decades of experience with the most challenging cases. We're here to help when routine endodontics isn't enough.
Mon-Fri: 8am-5pm | 23451 Madison St., Suite 210, Torrance, CA