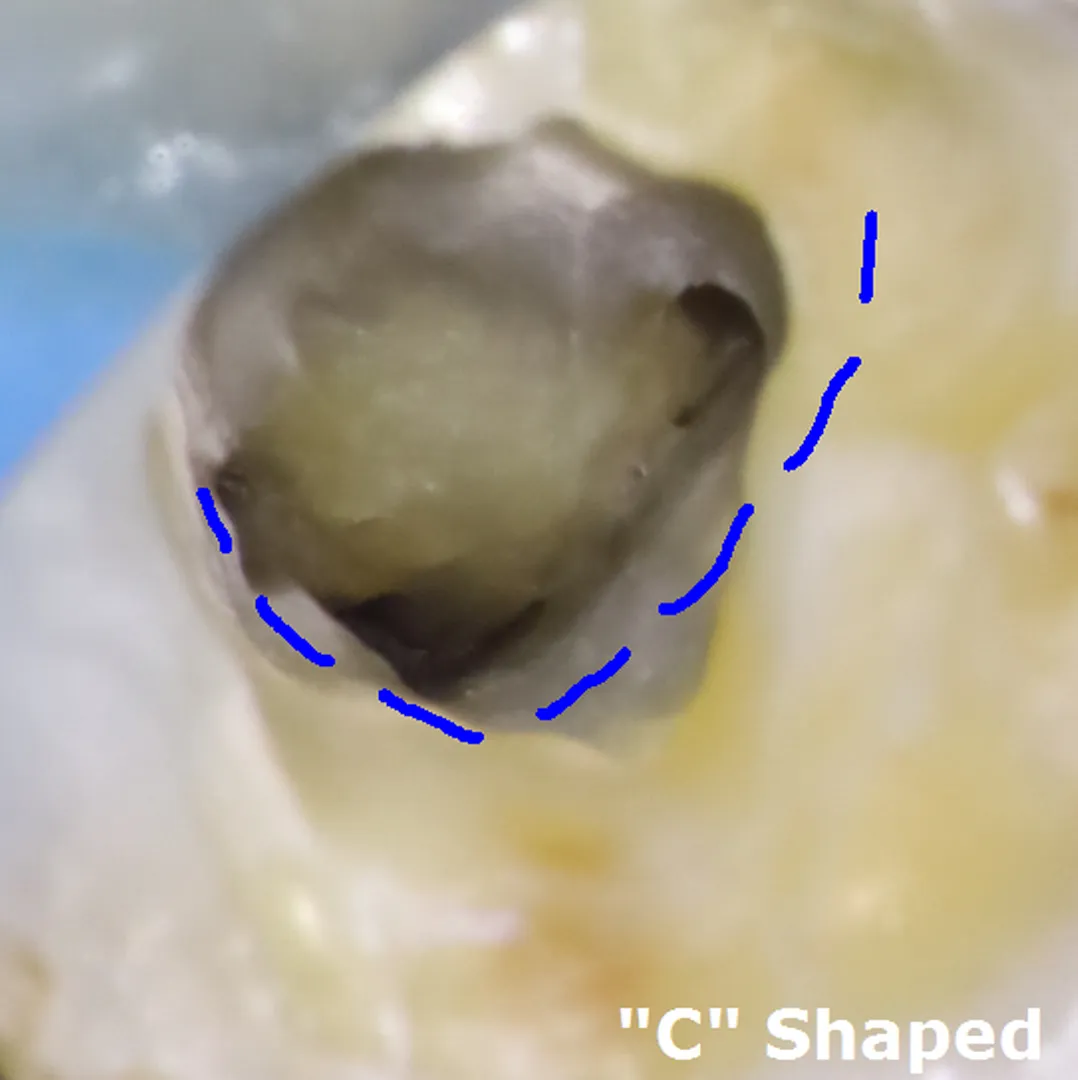
The C-shaped labyrinth.
Severe decay in a lower molar hid a rarity: no separate canals at all, but one continuous C-shaped ribbon of pulp — anatomy that defeats every standard technique.



One tooth's journey, in four beats.
A molar past warning.
A 51-year-old from Gardena with severe pain in a lower right second molar — no response to cold, deep decay on the film. His dentist sensed "something unusual" and referred before attempting treatment.
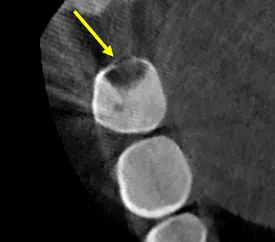
A ribbon, not rooms.
The CBCT revealed a Type I C-configuration: one continuous ribbon of pulp connecting what should be separate canals, with isthmus connections down the entire root.
A protocol redesigned.
A trapezoidal access instead of the standard triangle; circumferential filing along the C's walls instead of straight-line filing; GentleWave irrigation into fins no needle reaches. Ninety minutes.
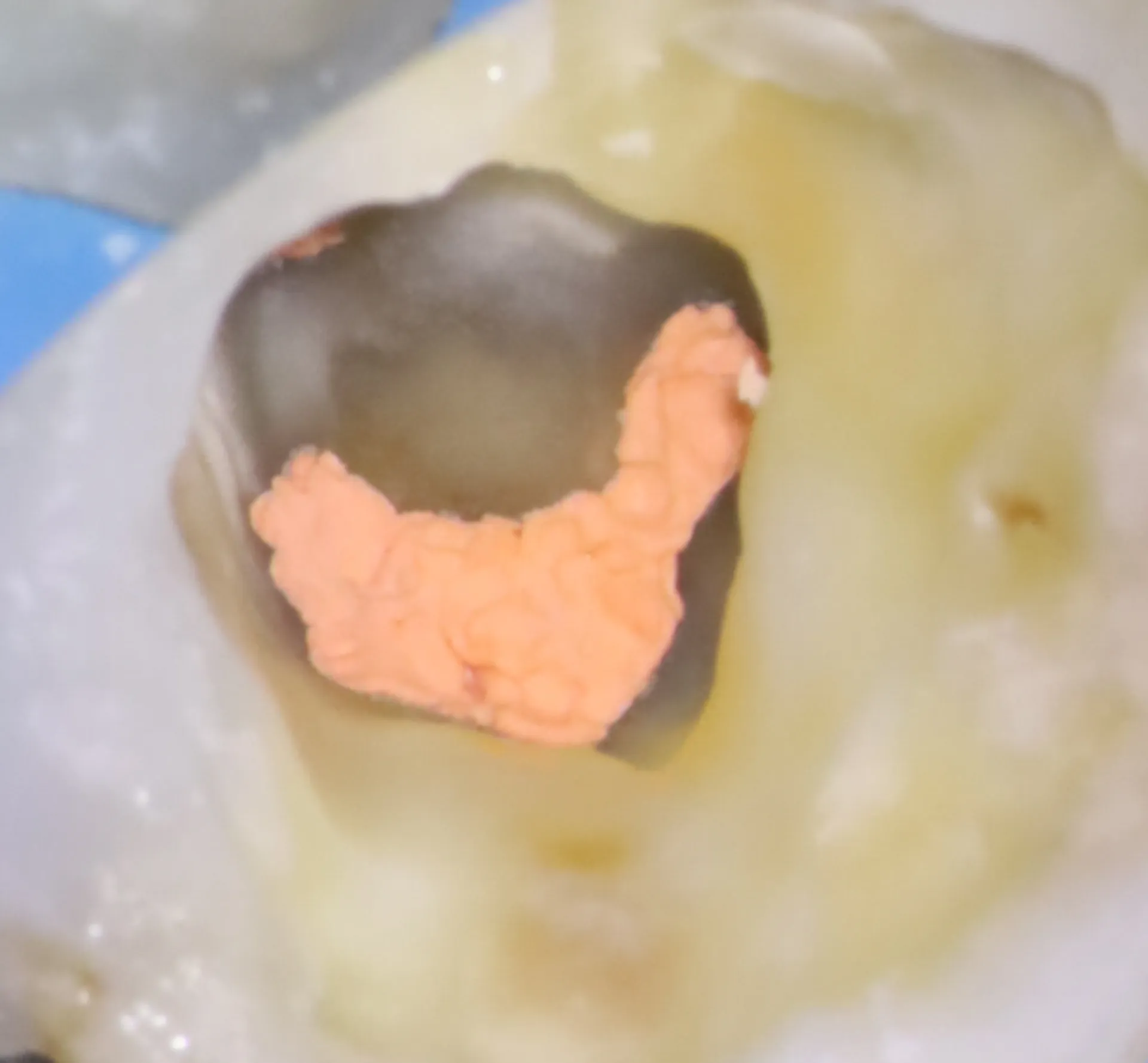
Sealed in three dimensions.
Warm, thermoplasticized filling shaped to the ribbon, an immediate biomimetic coronal seal on top — and the severe pain gone the same day.
- ✦ CBCT mapping of the Type I C-configuration before access
- ✦ Trapezoidal access cavity — not the standard triangle — to expose the full ribbon
- ✦ Circumferential filing along the inner and outer walls of the C
- ✦ GentleWave multisonic irrigation into the fins and isthmus connections
- ✦ Warm vertical compaction + multiple-cone technique to fill the irregular space
- ✦ Immediate biomimetic coronal seal
What this case teaches.
More from the collection.
- The canal that wasn't there — Two years of unexplained pain after a "finished" root canal — until 3D imaging revealed a fourth canal, sealed shut by calcification and invisible on every X-ray.
Told your tooth is "unusual"?
Unusual anatomy is our daily work. Get it mapped before anyone starts drilling.