
Beyond common causes like sinus pressure, muscle pain, and bruxism, there are neurological conditions that produce some of the most convincing imitations of dental pain. Trigeminal neuralgia stands out as particularly challenging — it can cause pain so intense and so tooth-specific that even experienced dentists may recommend root canal treatment on perfectly healthy teeth.
What Is Trigeminal Neuralgia?
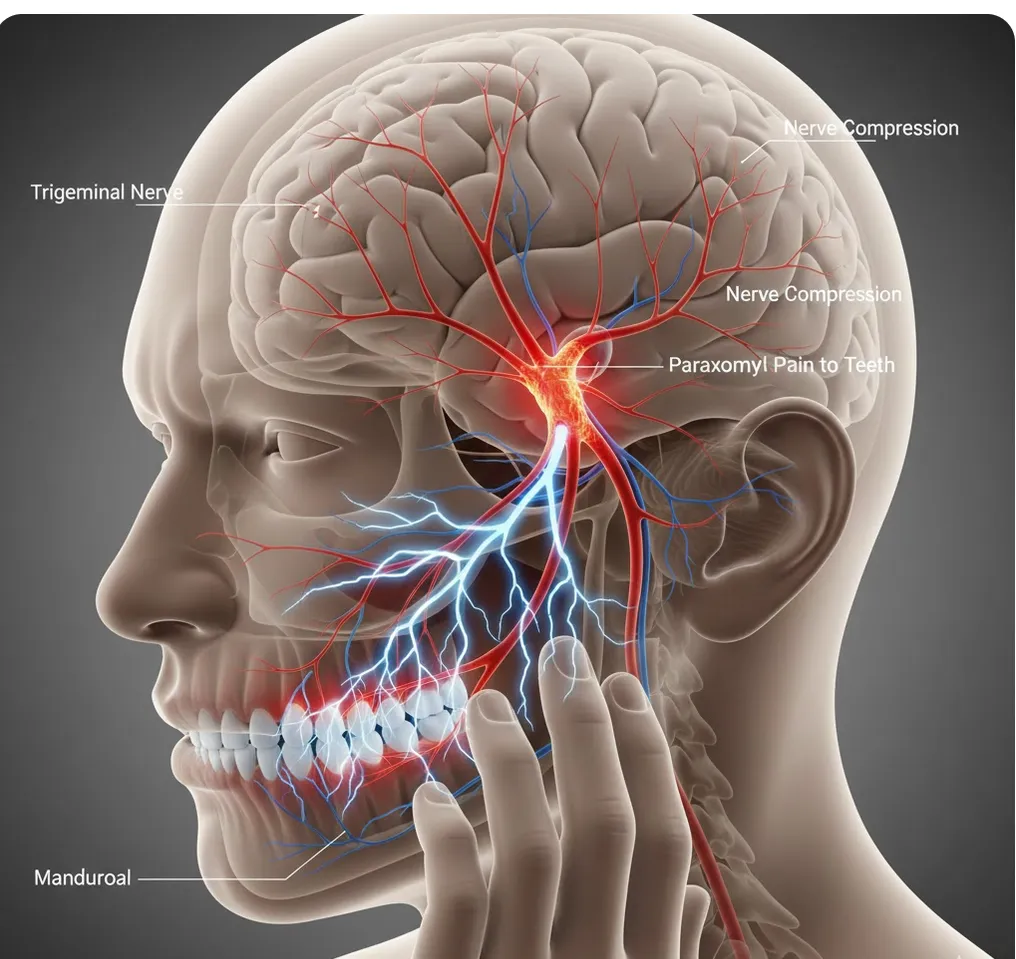
Trigeminal neuralgia is a neuropathic disorder affecting the trigeminal nerve, the main nerve responsible for sensation in the face, teeth, and jaws. It causes sudden, intense, electric-shock-like pain in the areas supplied by the nerve — which includes the teeth.
The trigeminal nerve has three branches:
- Ophthalmic (V1): Forehead, upper eyelid, scalp
- Maxillary (V2): Upper teeth, upper jaw, cheek, nose
- Mandibular (V3): Lower teeth, lower jaw, chin, tongue, lower lip
When trigeminal neuralgia affects the V2 or V3 branches, the pain can feel exactly like a severe toothache — sharp, stabbing, and localized to specific teeth. This is why it’s sometimes called the “suicide disease” due to the severity of the pain.
How Trigeminal Neuralgia Mimics Root Canal Pain
The symptoms can be remarkably convincing as dental problems:
- Intense, electric-shock-like pain in one or more teeth
- Pain triggered by light touch — brushing teeth, chewing, even a breeze on the face
- Episodes of severe, stabbing pain lasting seconds to minutes
- Pain localized to specific teeth or one side of the jaw
- Spontaneous pain that seems to come from nowhere
What makes trigeminal neuralgia so dangerous from a diagnostic standpoint is that the pain often appears to originate from a specific tooth. Patients point to the exact tooth that hurts, and the pain is severe enough that both patient and provider want to take action immediately.
Case Reports: Unnecessary Root Canals Before Correct Diagnosis
The dental literature documents multiple cases where patients underwent unnecessary root canal treatment before trigeminal neuralgia was recognized as the true cause:
- In two well-documented case reports, patients had root canals performed on healthy teeth before the diagnosis of trigeminal neuralgia was made. Once the correct diagnosis was established, carbamazepine therapy (an anticonvulsant medication) resolved the pain completely — no dental treatment was ever needed
- In another case series, space-occupying lesions such as tumors caused painful trigeminal neuropathy that presented as toothache, leading to dental treatments that were attributed to the wrong cause until MRI revealed intracranial pathology
These cases represent significant harm: irreversible dental procedures performed on healthy teeth, while the actual condition continued to worsen untreated.
The Malignancy Connection: Why Neurological Evaluation Matters
One of the most sobering findings from the research: reviews of mimicking lesions show that up to 43% are malignancies or metastases. This means that facial pain mimicking a toothache can sometimes be the first sign of a serious condition — a tumor pressing on or invading the trigeminal nerve.
This statistic underscores why a comprehensive diagnostic approach is not optional. When dental evaluation finds no cause for the pain, the next step must be neurological evaluation with appropriate imaging (MRI), not another dental procedure.
Other Neurological Conditions That Mimic Dental Pain
Trigeminal neuralgia isn’t the only nerve condition that can fool dentists:
Shingles (Herpes Zoster)
The varicella-zoster virus can reactivate along the trigeminal nerve, causing severe tooth and jaw pain before any rash appears. We’ve written extensively about this — read our full guide on shingles presenting as tooth pain.
Postherpetic Neuralgia
After a shingles outbreak, chronic nerve pain can persist for months or years, continuing to mimic toothache long after the rash has healed.
Atypical Odontalgia (Persistent Dentoalveolar Pain)
A chronic pain condition where patients experience persistent tooth pain despite no identifiable dental cause and normal test results. This condition may follow dental procedures or appear spontaneously.
Referred Pain from Intracranial Pathology
Tumors, aneurysms, or other structural abnormalities affecting the trigeminal nerve pathway can produce pain that localizes to the teeth and jaw.
Warning Signs That Your Pain May Be Neurological
Symptoms Pointing Toward Trigeminal Neuralgia
- Pain is sudden, severe, and electric-shock-like — not the typical dull ache of a toothache
- Episodes are brief (seconds to two minutes) but extremely intense
- Pain is triggered by light touch — brushing teeth, washing face, eating, or a light breeze
- There are pain-free intervals between attacks
- Pain stays on one side of the face and follows a nerve distribution pattern
- No dental cause found despite thorough examination
Dental Tests That Rule Out Tooth Problems
- Teeth respond normally to vitality testing
- CBCT 3D imaging shows no periapical pathology, decay, or fractures
- Pain does not respond to local anesthesia in the typical way
- Previous dental treatment has not resolved the pain
Symptoms pointing toward other neurological causes
- Pain is paroxysmal (comes in sudden bursts) and does not respond to dental treatment
- Progressive worsening over weeks or months
- Numbness or tingling accompanying the pain
- Associated neurological symptoms (vision changes, weakness, difficulty swallowing)
Why a Detailed Consultation Matters More Than a Free One
Neurological conditions that mimic dental pain are among the most commonly misdiagnosed causes of tooth pain. This makes the quality of your initial consultation critically important.
You may see “free consultation” offers on sponsored Google ads when looking for a root canal dentist in Torrance. But a consultation without CBCT 3D imaging, comprehensive vitality testing, and a provider trained in differential diagnosis of orofacial pain is unlikely to catch a neurological condition masquerading as a toothache.
The consequences of misdiagnosis here are severe: irreversible dental procedures on healthy teeth, while a potentially serious neurological condition goes undiagnosed and untreated. In the case of tumors causing trigeminal neuropathy, delayed diagnosis can be life-altering.
At our office, 30% of consultations reveal that the pain source is non-dental, saving patients from unnecessary procedures. Our comprehensive consultation includes advanced CBCT 3D imaging, pulp vitality testing, and the clinical expertise to recognize when pain doesn’t fit a dental pattern — and when to refer for neurological evaluation.
A thorough consultation isn’t just about saving money on unnecessary procedures — it can be the difference between catching a serious condition early and missing it entirely. See what our consultation includes.
The Endodontist’s Role in Neurological Pain
As endodontists in Torrance, we are trained to identify when tooth pain has a non-dental origin. For patients whose pain may be neurological, our diagnostic protocol includes:
- CBCT 3D imaging to definitively rule out dental pathology
- Pulp vitality testing (cold test, electric pulp test) to confirm healthy teeth
- Selective anesthesia to determine whether blocking specific teeth eliminates the pain
- Pain pattern analysis — recognizing when pain characteristics don’t match dental disease
- Appropriate referral to neurologists, ENT specialists, or orofacial pain specialists when a non-dental cause is suspected
Our goal is to give patients a definitive answer: either the tooth is the problem and we treat it, or it isn’t, and we guide you to the right provider. Either way, you leave with clarity.
Key Takeaways
- Trigeminal neuralgia causes severe, electric-shock-like facial pain that is frequently misdiagnosed as a dental problem
- Case reports document patients receiving unnecessary root canals before the correct neurological diagnosis was made
- Up to 43% of mimicking lesions are malignancies — making neurological evaluation critical for unexplained facial pain
- Other conditions including shingles, postherpetic neuralgia, and intracranial pathology can also mimic dental pain
- Comprehensive testing — CBCT imaging, vitality tests, and clinical expertise — is essential for accurate diagnosis
- If pain is sudden, stabbing, and triggered by light facial touch, seek neurological evaluation alongside dental assessment
Experiencing Severe, Unexplained Facial Pain?
If you’re dealing with intense tooth or facial pain that hasn’t responded to dental treatment, or if previous evaluations haven’t found a clear dental cause, a specialist evaluation is the next step. At Phan Endodontic Partners in Torrance, we use CBCT 3D imaging and advanced diagnostic protocols to determine whether your pain is dental or requires neurological evaluation.
Call (310) 378-8342 to schedule a consultation.