Fractured Front Tooth Saved — Retreatment Case

Patient Profile
62-year-old Redondo Beach patient with fractured maxillary central incisor and failed previous root canal treatment
Clinical Challenge
Compromised tooth structure with inadequate previous endodontic treatment—extraction and implant seemed inevitable
Approach
Endodontic retreatment, fiber post placement, and composite buildup to preserve natural tooth
Outcome
Tooth saved and functional at 1-year recall with full crown restoration
The Second Opinion Decision
This 62-year-old patient presented with a fractured maxillary central incisor and a previous root canal treatment that had failed. Another provider had recommended extraction and implant placement—a reasonable suggestion given the extent of tooth structure loss and endodontic failure.
But the patient wasn't ready to give up on their natural tooth. They sought a second opinion to explore whether the tooth could be saved. This case demonstrates the value of specialist evaluation before committing to extraction.
Clinical Assessment
Initial examination revealed:
- Fractured crown: Significant coronal tooth structure lost due to fracture
- Failed endodontic treatment: Radiograph showed inadequate root canal obturation with voids and short fill
- Residual root structure: Sufficient remaining tooth structure below gingival level for potential restoration
- No apical pathology: Periapical tissues appeared healthy despite treatment deficiencies
- Strategic importance: Central incisor—losing it creates significant aesthetic and functional deficit
Treatment vs. Extraction: The Decision Matrix
We weighed several factors when considering tooth preservation:
Factors Favoring Extraction/Implant:
- Significant loss of coronal tooth structure
- Previous endodontic failure suggesting difficult anatomy or poor seal
- Age of patient (62)—implants typically work well in older adults
- Predictable outcome with modern implant dentistry
Factors Favoring Tooth Preservation:
- Adequate root length and remaining structure for post and core
- Patient strongly preferred keeping natural tooth
- No active infection or periapical pathology
- Avoiding implant surgery, bone grafting, and extended treatment timeline
- Natural tooth proprioception and periodontal ligament maintained
- Cost considerations—retreatment and post/core typically less expensive than implant
The Evidence for Saving Compromised Anterior Teeth
Recent research supports attempting to save extensively compromised anterior teeth when sufficient root structure remains. Studies show fiber posts significantly increase fracture resistance of endodontically treated anterior teeth, particularly when combined with full coverage crowns.
Systematic reviews demonstrate that fiber post placement can improve fracture strength when at least moderate tooth structure loss is present. The key is proper retreatment technique and adequate ferrule (sound tooth structure extending coronally from the margin).
Treatment Protocol
The 90-minute appointment focused on three sequential objectives: (1) endodontic retreatment to create proper seal, (2) fiber post placement for intraradicular reinforcement, and (3) composite buildup to restore coronal form.
Phase 1: Endodontic Retreatment
- Access and Removal (Minutes 0-20):
- Remove fractured coronal segment and compromised tooth structure
- Access existing root canal treatment under magnification
- Remove inadequate gutta-percha obturation material using solvents and ultrasonic instruments
- Locate canal orifice and verify patency to apex
- Cleaning and Shaping (Minutes 20-50):
- Establish working length with electronic apex locator and radiographic verification
- Instrument canal using rotary NiTi files to remove contaminated dentin
- Irrigate thoroughly with sodium hypochlorite to disinfect canal system
- Passive ultrasonic irrigation to enhance cleaning of apical anatomy
- Obturation (Minutes 50-60):
- Dry canal with paper points
- Obturate with warm vertical compaction gutta-percha technique
- Verify complete fill with radiograph—no voids or short fills
- Place temporary seal over canal orifice
Phase 2: Fiber Post Placement (Minutes 60-75)
After achieving proper endodontic seal, intraradicular reinforcement was needed due to minimal remaining coronal structure:
- Post space preparation: Remove gutta-percha from coronal 2/3 of canal, leaving 4-5mm apical seal
- Post selection: Choose fiber post diameter matching prepared post space
- Post try-in: Verify post extends adequately into canal and provides sufficient length for core buildup
- Adhesive cementation: Bond fiber post using dual-cure resin cement with total-etch adhesive protocol
Why Fiber Posts vs. Metal Posts
Recent literature strongly favors fiber-reinforced posts over traditional metal posts for anterior teeth:
- Similar elastic modulus to dentin: Fiber posts flex with tooth structure rather than creating stress concentrations
- Lower risk of catastrophic root fracture: Metal posts can cause vertical root fractures that render tooth unrestorable
- Adhesive bonding: Fiber posts bond to tooth structure; metal posts rely on retention alone
- Retrievability: If retreatment needed, fiber posts can be removed; metal posts often require extraction
- Aesthetics: Fiber posts don't show through translucent anterior crowns
Phase 3: Composite Buildup (Minutes 75-90)
Final phase restored coronal tooth anatomy:
- Build composite core around fiber post using layering technique
- Restore anatomic contours to prepare for eventual crown
- Ensure adequate ferrule (2mm of sound tooth structure for crown margin)
- Refine margins and polish buildup
- Place temporary crown for protection and aesthetics
- Schedule with restorative dentist for definitive crown in 2-3 weeks
Critical Success Factors
This case succeeded because:
- Adequate remaining root structure for post retention and ferrule
- Proper retreatment technique with thorough disinfection and complete obturation
- Fiber post bonded adhesively for reinforcement without stress concentration
- Immediate buildup and temporization to protect restored tooth
- Definitive crown placement for long-term strength and seal
Evidence-Based Outcomes
Research Supporting Tooth Preservation
Multiple systematic reviews and meta-analyses published in 2024-2025 provide robust evidence for this treatment approach:
Endodontic Retreatment Success
- Overall success rates: 83% success-survivor rate for retreatment teeth, even in cases with complications
- Anterior teeth specifically: Higher success rates than posterior teeth due to simpler anatomy and easier access
- Factors improving success: Microscope use, thorough cleaning, complete obturation to apex
Fiber Post Performance in Anterior Teeth
Recent meta-analyses demonstrate clear benefits of fiber posts:
- Fracture resistance: Fiber posts significantly increase fracture resistance of endodontically treated anterior teeth compared to no post
- Greatest benefit: When at least moderate tooth structure loss (two or more Class III/IV restorations)
- Post length: Minimum 2/3 of root length or equal to crown length, whichever is greater
- Combined with crowns: Full coverage crowns dramatically improve long-term survival (97% survival vs. 68% without crown)
Fracture Strength After Retreatment
One concern with retreatment is weakening tooth structure. Research shows:
- Endodontically retreated teeth may present slightly lower fracture strength than initially treated teeth
- However, proper post-and-core restoration and full crown largely compensate for this reduction
- The difference is clinically insignificant when adequate ferrule and full coverage restoration are present
This Case at 1-Year Follow-Up
At one-year recall, the tooth demonstrated:
- Asymptomatic function: No pain, sensitivity, or discomfort
- Radiographic success: No periapical radiolucency, stable bone levels
- Intact restoration: Full coverage crown showing no signs of failure
- Normal mobility: Physiologic mobility consistent with healthy periodontal ligament
- Patient satisfaction: Highly satisfied with decision to save natural tooth
- Aesthetic success: Tooth matches adjacent central incisor in color, contour, and translucency
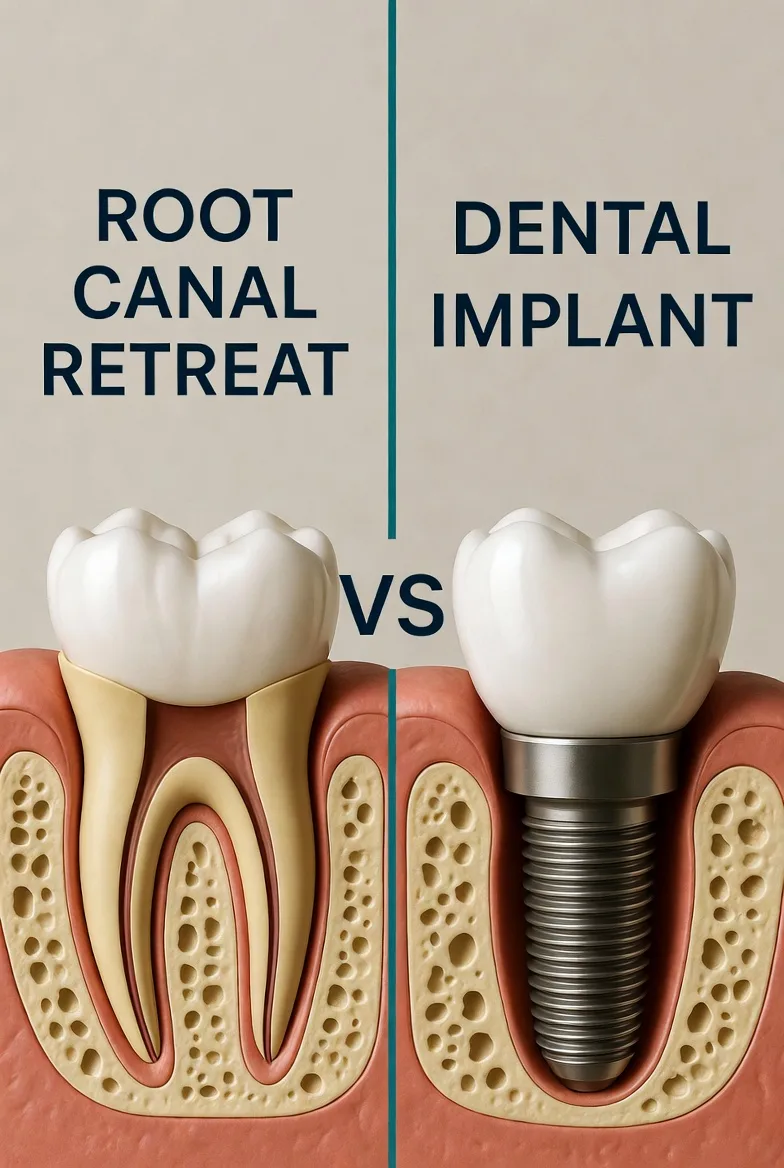
Comparison to Implant Alternative
If extraction and implant placement had been chosen instead:
- Timeline: 6+ months (extraction, healing, bone graft if needed, implant placement, healing, crown)
- Surgical procedures: Extraction, possible bone grafting, implant surgery (vs. one endodontic visit)
- Cost: Typically 2-3x higher for implant than retreatment + post/core + crown
- Proprioception: Natural tooth maintains periodontal ligament proprioception; implant does not
- Reversibility: If this treatment had failed, extraction and implant still remained as backup option
Research sources cited: Evidence from systematic reviews shows fiber posts increase fracture resistance (PubMed 33546858), retreatment success rates around 83% (PMC11276083), and full crown placement improves survival to 97% for compromised teeth (PubMed 33103524).
Key Takeaways
Clinical Decision-Making
- Second opinions have value: What seems like a hopeless tooth to one provider may be salvageable with specialist intervention. Patients benefit from exploring all options before committing to extraction.
- Not every failed case needs extraction: Endodontic retreatment, even in fractured teeth, can be successful with proper technique and adequate remaining tooth structure.
- Fiber posts are modern standard of care: Superior to metal posts for anterior teeth in every measurable way—fracture resistance, aesthetics, retrievability, and stress distribution.
- The ferrule principle is critical: Minimum 2mm of sound tooth structure coronal to bone level is essential for long-term success of crowned teeth.
- Crowns are mandatory for fractured teeth: Composite buildups alone will fail. Full coverage crowns distribute occlusal forces and prevent further fracture propagation.
When to Attempt Tooth Preservation
Saving compromised anterior teeth is appropriate when:
- Adequate root length remains (at least 2/3 of original length)
- Sufficient ferrule can be achieved (2mm of sound tooth structure above bone)
- No vertical root fracture present (catastrophic and unrestorable)
- Patient understands treatment may not succeed and extraction remains backup option
- Patient willing to invest in both endodontic treatment and definitive crown
When Extraction is the Better Choice
Recommend extraction and implant when:
- Vertical root fracture present (tooth is unrestorable)
- Insufficient remaining root structure for post retention
- Unable to achieve adequate ferrule (crown will fail without it)
- Severe root resorption or advanced periodontal disease
- Patient prefers predictable implant over uncertain tooth preservation
Evidence-Based Practice
Modern research clearly supports attempting to preserve natural teeth when favorable conditions exist. The 83% success rate for endodontic retreatment, combined with 97% survival for crowned teeth with adequate ferrule, makes tooth preservation a viable first-line treatment for many compromised anterior teeth.
Bottom Line: Don't assume extraction and implant is the only option for fractured anterior teeth with failed root canals. Specialist evaluation can identify cases where retreatment, post-and-core buildup, and crown restoration offer excellent prognosis for natural tooth preservation.
Clinical Disclaimer: These cases are presented for educational purposes and published with appropriate patient consent. Patient identifying information has been removed in compliance with HIPAA regulations. Individual results may vary. All radiographic images and case descriptions represent actual patient treatment outcomes.
Procedures We Use for These Cases
The expertise demonstrated in these cases comes from mastering advanced endodontic procedures
Cracked Tooth Treatment in Torrance, CA
Expert cracked tooth diagnosis and repair in Torrance. Dr. Jason Phan uses CBCT 3D imaging, microscope visualization, and biomimetic bonding to save cracked teeth.
Learn moreRoot Canal Retreatment in Torrance, CA
Failed root canal? Dr. Jason Phan specializes in root canal retreatment in Torrance using CBCT imaging and microscope technology to save teeth other dentists can't.
Learn moreRelated Articles
Learn more about these treatments from Dr. Phan
 Cracked Teeth
Cracked Teeth Cracked Tooth: Crown, Root Canal, or Extraction? How We Decide
Not all cracked teeth need the same treatment. Dr. Jason Phan explains the 5 types of cracks, which ones can be saved, and how a microscope and CBCT determine the right treatment.
 Surgery & Retreatment
Surgery & Retreatment Retreatment vs. Apicoectomy: Which Fixes a Failed Root Canal?
Failed root canal — should you redo it or go straight to surgery? Dr. Jason Phan compares retreatment vs. apicoectomy: when each works, success rates, costs, and recovery.
 Surgery & Retreatment
Surgery & Retreatment Failed Root Canal: Should You Try Retreatment or Get an Implant?
Your root canal didn't work — now what? Dr. Jason Phan compares retreatment vs. extraction and implant: success rates, costs, timelines, and how to decide which is right for your tooth.
 Root Canal
Root Canal Persistent Pain After Root Canal: Causes, Evidence, and When Retreatment Is Needed
A detailed clinical guide to understanding why pain persists after root canal treatment. Dr. Jason Phan covers odontogenic and nonodontogenic causes, diagnostic approaches, and evidence from current research.
Surgery & Retreatment Root Canal Retreatment: When Your First Root Canal Fails
Your root canal didn't work. Now what? Dr. Jason Phan explains why root canals fail, what retreatment involves, and when it's worth saving the tooth.
Cracked Teeth Cracked Tooth Symptoms: When to See an Endodontist in Torrance
How do you know if your tooth is cracked? Dr. Jason Phan explains the symptoms of a cracked tooth, why they're tricky to diagnose, and when you need specialist help in Torrance.
 Root Canal
Root Canal Root Canal Pain After Treatment: What's Normal and What's Not
Some discomfort after a root canal is normal, but how do you know if something is wrong? Dr. Jason Phan explains what to expect during recovery, warning signs to watch for, and when to call your endodontist.
 Pain Diagnosis
Pain Diagnosis Bruxism Pain Mimicking Root Canal Pain: When Grinding Feels Like a Toothache
Teeth grinding and clenching can cause tooth pain that mimics root canal symptoms. Dr. Jason Phan explains how a CBCT consultation in Torrance prevents unnecessary treatment.
Experience Matters in Complex Endodontics
When you refer patients to us, they benefit from decades of experience with the most challenging cases. We're here to help when routine endodontics isn't enough.
Mon-Fri: 8am-5pm | 23451 Madison St., Suite 210, Torrance, CA