Perforation Repair with MTA — Saving a Damaged Molar
Patient Profile
68-year-old Carson resident referred for saving
Clinical Challenge
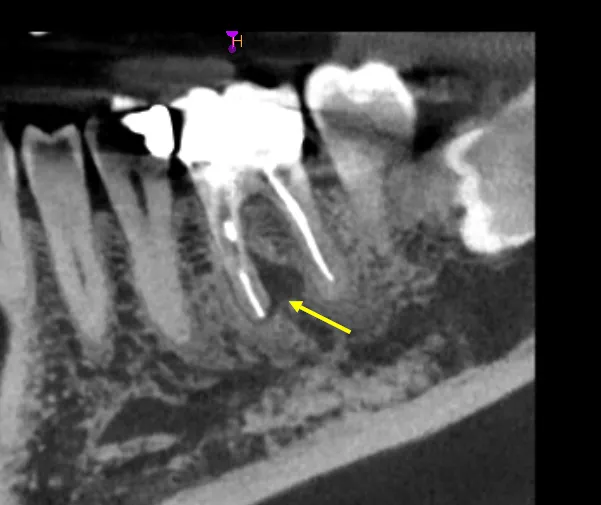
Large furcation perforation with active bleeding—high risk of periodontal communication and treatment failure if not addressed
Approach
MTA repair under microscope, followed by completion of endodontic treatment once perforation sealed
Outcome
Perforation successfully sealed, canals completed, tooth asymptomatic
Treatment Details
Perforations are one of the most common iatrogenic complications in endodontics. This patient's general dentist made the right decision: stop immediately, don't attempt to "fix it yourself," and refer to a specialist the same day. Delay in perforation repair dramatically worsens prognosis as bacteria colonize the defect and periodontal breakdown accelerates.
The referring dentist had searched for the distal canal, drilled too far lingually, and created a 2mm perforation directly into the furcation. The patient presented with active bleeding from the perforation site and understandable anxiety about losing the tooth.
Perforation Repair Protocol
- Hemostasis First: Control bleeding with calcium chloride-soaked pellets—you cannot repair what you cannot see
- Perforation Isolation: Create a "dry field" using microscope magnification and careful bleeding control
- MTA Placement: Pack mineral trioxide aggregate into perforation defect under high magnification
- Setting Time: Allow 48-72 hours for MTA to fully set before continuing treatment
- Complete Endodontics: Return to complete canal treatment once perforation sealed
Why MTA Works
Mineral trioxide aggregate has unique properties for perforation repair:
- Biocompatible: Tissues tolerate direct contact with MTA
- Antibacterial: High pH creates hostile environment for bacteria
- Sets in moisture: Works even with blood contamination (though dry is better)
- Dimensionally stable: Doesn't shrink or expand after setting
- Seals effectively: Creates hermetic seal preventing bacterial leakage
Timing is Critical
Perforation repair outcomes correlate directly with time to treatment:
- Immediate (same day): 90% success rate
- Within 1 week: 70-80% success rate
- After 1 month: 50% success rate or less
This patient was treated within 3 hours of perforation—optimal timing for repair success.
Clinical Assessment
This case demonstrates why immediate specialist referral after perforation is essential. The general dentist's decision to stop immediately and refer rather than attempting to continue saved this tooth. Many perforations become unresolvable because well-intentioned attempts to "finish the case" contaminate the defect and allow periodontal breakdown.
Prognostic Factors for Perforation Repair
Success depends on several factors:
- Size: Smaller perforations (<2mm) heal better than large defects
- Location: Coronal perforations worse than apical; furcation perforations challenging but salvageable
- Time to Repair: Immediate repair far superior to delayed
- Contamination: Clean perforations heal better than those exposed to oral bacteria
- Hemostasis: Adequate bleeding control during repair improves seal quality
Long-Term Outcome
At 3-year follow-up, this tooth shows excellent healing:
- Radiographic evidence of bone maintenance at perforation site
- Normal periodontal probing depths (no pocket formation)
- No symptoms, no sensitivity
- Tooth functional with crown in place
Alternative Would Have Been Extraction
Without immediate repair, this perforation would have led to:
- Progressive periodontal bone loss at furcation
- Persistent infection despite canal treatment
- Treatment failure within 6-12 months
- Eventual extraction and implant placement
Key Takeaways
Clinical Insights
- Stop immediately when perforation occurs: Don't try to finish the case. Every minute of contamination worsens prognosis.
- Same-day referral is ideal: Call the specialist while the patient is still in your chair. Immediate repair has 90% success rates.
- Bleeding is not your enemy—it's information: Active bleeding from unexpected locations indicates perforation. Don't ignore it.
- MTA is the gold standard: Older materials (amalgam, composite, IRM) don't perform as well for perforation repair. MTA's biocompatibility and sealing ability are superior.
- Microscopes prevent perforations: Most perforations occur when working blind. Magnification and proper lighting dramatically reduce iatrogenic errors.
Preventing Perforations
- Use pre-operative CBCT for complex anatomy
- Work under magnification (loupes minimum, microscope ideal)
- Know the expected anatomical locations of canal orifices
- Use non-cutting pilot burs initially for access
- If you encounter bleeding where you don't expect it, stop and reassess
- When searching for canals, use conservative troughing rather than aggressive drilling
When to Refer vs. Extract
Refer for attempted repair when:
- Perforation is recent (same day to one week)
- Perforation is <3mm in diameter
- No significant periodontal breakdown yet visible
- Tooth has adequate crown structure for restoration
Consider extraction when:
- Perforation is large (>4mm) or involves multiple areas
- Perforation has been present for months with established periodontal defect
- Tooth has insufficient structure for functional restoration
- Patient prefers implant over attempting uncertain repair
Bottom Line: Perforations are complications, not catastrophes—if treated immediately. The referring dentist's prompt action saved this tooth. Delay would have made it unsalvageable.
Clinical Disclaimer: These cases are presented for educational purposes and published with appropriate patient consent. Patient identifying information has been removed in compliance with HIPAA regulations. Individual results may vary. All radiographic images and case descriptions represent actual patient treatment outcomes.
Procedures We Use for These Cases
The expertise demonstrated in these cases comes from mastering advanced endodontic procedures
Root Canal Retreatment in Torrance, CA
Failed root canal? Dr. Jason Phan specializes in root canal retreatment in Torrance using CBCT imaging and microscope technology to save teeth other dentists can't.
Learn moreEndodontic Surgery & Microsurgery in Torrance
Expert endodontic microsurgery and apicoectomy in Torrance. Minimally invasive surgical procedures using 25x microscopic magnification when traditional root canal treatment isn't enough.
Learn moreRelated Articles
Learn more about these treatments from Dr. Phan
 Surgery & Retreatment
Surgery & Retreatment Retreatment vs. Apicoectomy: Which Fixes a Failed Root Canal?
Failed root canal — should you redo it or go straight to surgery? Dr. Jason Phan compares retreatment vs. apicoectomy: when each works, success rates, costs, and recovery.
 Surgery & Retreatment
Surgery & Retreatment Failed Root Canal: Should You Try Retreatment or Get an Implant?
Your root canal didn't work — now what? Dr. Jason Phan compares retreatment vs. extraction and implant: success rates, costs, timelines, and how to decide which is right for your tooth.
 Root Canal
Root Canal Persistent Pain After Root Canal: Causes, Evidence, and When Retreatment Is Needed
A detailed clinical guide to understanding why pain persists after root canal treatment. Dr. Jason Phan covers odontogenic and nonodontogenic causes, diagnostic approaches, and evidence from current research.
 Surgery & Retreatment
Surgery & Retreatment Apicoectomy Explained: When Root Canal Isn't Enough
Sometimes a root canal isn't enough to save a tooth. Dr. Jason Phan explains what an apicoectomy is, when you need one, and what to expect during recovery.
Surgery & Retreatment Root Canal Retreatment: When Your First Root Canal Fails
Your root canal didn't work. Now what? Dr. Jason Phan explains why root canals fail, what retreatment involves, and when it's worth saving the tooth.
 Root Canal
Root Canal Root Canal Pain After Treatment: What's Normal and What's Not
Some discomfort after a root canal is normal, but how do you know if something is wrong? Dr. Jason Phan explains what to expect during recovery, warning signs to watch for, and when to call your endodontist.
Experience Matters in Complex Endodontics
When you refer patients to us, they benefit from decades of experience with the most challenging cases. We're here to help when routine endodontics isn't enough.
Mon-Fri: 8am-5pm | 23451 Madison St., Suite 210, Torrance, CA