Scheduled for extraction, still here.
Another provider said the tooth had to go — a perforation, a draining sinus tract, a root canal that had failed. Five years after combined retreatment and surgical repair, it's still doing its job.




One tooth's journey, in four beats.
The extraction was already recommended.
The tooth had a perforation, a sinus tract draining infection from the bone, and a root canal that hadn't resolved the problem. The recommendation to extract wasn't unreasonable. The patient wanted one more opinion before losing the tooth.
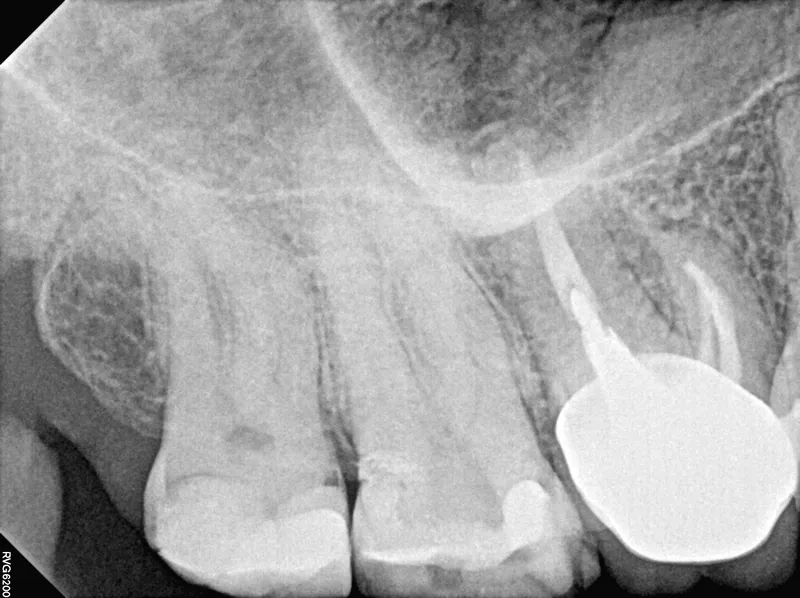
At the edge — not past it.
Imaging showed the perforation defect, anatomy the first treatment never reached, and persistent infection. The combination put the tooth at the edge of what's salvageable. Edge is not past. We saw a path, and we were honest about the odds.
Two procedures, one save.
First, non-surgical retreatment: the missed anatomy located, disinfected, medicated, and sealed. Then the surgical phase: a small flap, the diseased tissue removed, and both the root end and the perforation repaired with MTA — a bioceramic that bonds to dentin and supports the bone growing back.
Five years, still working.
Recalls at two months, one year, three years, and five years. Bone filled in around the repaired root, the sinus tract never returned, and the tooth another provider had scheduled for extraction is still in normal function.
- ✦ Second-opinion consultation with CBCT before any irreversible decision
- ✦ Non-surgical retreatment — previously missed anatomy located and disinfected
- ✦ Calcium hydroxide medication between visits; obturation to length
- ✦ Surgical phase — flap access, curettage of the infected tissue
- ✦ Root-end resection and MTA seal; perforation repaired with MTA
- ✦ Recalls at 2 months, 1 year, 3 years, and 5 years — progressive bone fill at each
What this case teaches.
More from the collection.
- Out, repaired, and home again — A failing root canal locked behind a large metal post — unreachable from above, impractical from the side. So the tooth came out, was repaired in fifteen minutes, and went back in.
- Sealing the wrong turn — A drill searching for a canal went 2mm past where it should have — straight into the furcation. Three hours later the hole was sealed, and three years later the tooth is still here.
- Six problems, one tooth — A failing root canal hiding a separated file, a calcified canal, a missed canal, internal resorption, and a crack — quiet and healed 3.4 years after retreatment.
Told your tooth has to come out?
Bring the X-rays. A second opinion is a conversation, not a commitment — and sometimes it changes everything.