
It's the fork every infected tooth arrives at: repair the original, or remove and replace it. The dental internet argues about this endlessly; in the chair, the decision follows a fairly clear ledger. Here it is — including the cases where extraction honestly wins.
| FACTOR | FAVORS SAVING | FAVORS EXTRACTION |
|---|---|---|
| Structure | Enough sound tooth to rebuild on | Decay or fracture below the bone line |
| The root | Intact, treatable canals | Vertical root fracture |
| Bone support | Healthy periodontal foundation | Severe, uncontrolled gum disease |
| Cost | $2,100–$3,500 (root canal + crown) | $4,000–$6,000+ with implant |
| Timeline | 2–3 appointments over 2–4 weeks | 4–9 months of healing and stages |
| Success rate | 90–97% for specialist root canals | ~95% for implants, but more complex |
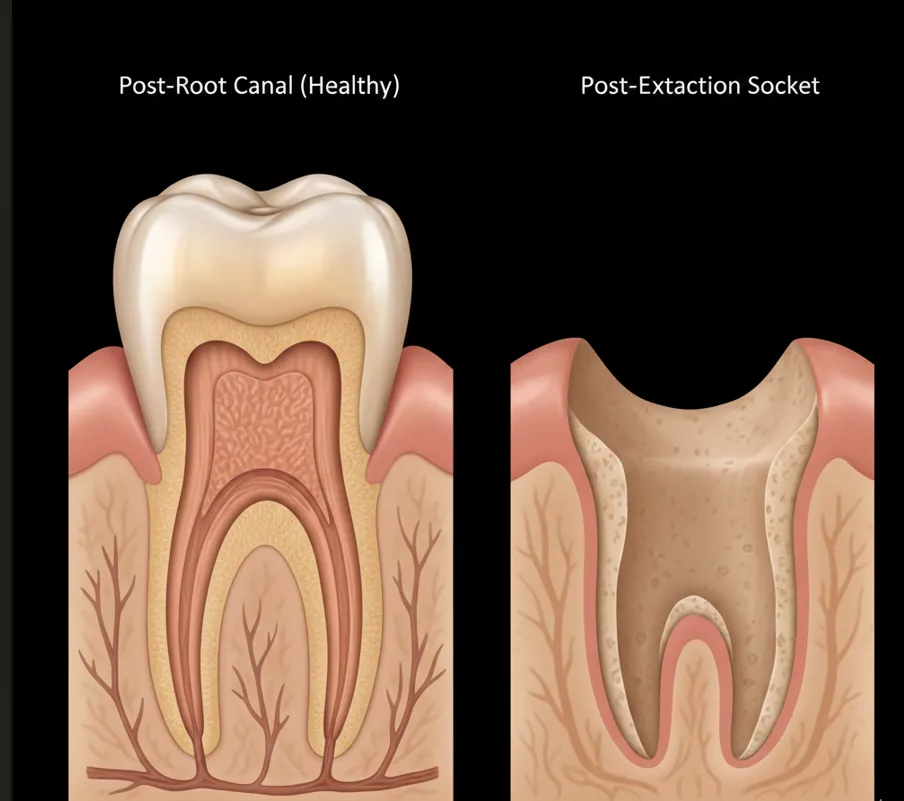
| Biology | Your own ligament, sensation, bone stimulus | Titanium — excellent, but not alive |
Why the tie goes to the tooth.
A natural tooth does things no implant replicates: it feels pressure through a periodontal ligament that absorbs chewing forces, flexes with the jaw, and keeps the surrounding bone stimulated and alive. Success rates for specialist root canals run 90–97% — comparable to implants — at a fraction of the cost and time. The root canal and crown complete the treatment in weeks; an implant means surgery to place the post, 3–6 months of healing, then a second procedure for the crown. When the odds are close, keeping the original is the conservative bet.
Saving a tooth now doesn’t prevent extraction later. If a root canal doesn’t work out, you can still extract the tooth and place an implant. But if you extract first, you can never get that natural tooth back.
When extraction honestly wins.
A vertically fractured root. A tooth decayed past the point of rebuilding. A foundation lost to severe, uncontrolled gum disease. A tooth that’s failed both root canal and retreatment (though apicoectomy is worth considering first). In those cases a root canal is money spent on a tooth with no future — and we say so plainly, because a well-planned implant beats a doomed save every time.
One important note: these determinations require proper diagnosis with adequate imaging. What looks like a hopeless tooth on a 2D X-ray may turn out to be saveable when evaluated with 3D CBCT imaging and a microscope. Our case files include both kinds of honesty: a “hopeless” tooth saved, and consultations where we advised against our own procedure.
How the decision is actually made.
Microscope examination
Evaluating tooth structure, cracks, and condition under 25x magnification.
CBCT 3D imaging
Assessing the roots, bone, and any infection in detail that standard X-rays can't show.
Vitality testing
Determining the current state of the tooth's nerve — cold, percussion, bite, palpation.
Honest assessment
We tell you whether the tooth is saveable, what the prognosis is, and what we'd do if it were our own tooth. If extraction is the better option, we say so directly.
Structurally sound tooth, treatable root, healthy foundation: save it — the biology and the economics both agree. Fractured, hollowed, or unsupported: replace it well.
The decision needs imaging, not ideology. Thirty minutes and a scan give you the honest answer for your specific tooth.